Requirements of the Americans with Disabilities Act
One of the primary responsibilities of state and local governments is to protect residents and visitors from harm, including assistance in preparing for, responding to, and recovering from emergencies and disasters, to include public health emergencies. State and local governments must comply with Title II of the ADA in the emergency- and disaster-related programs, services, and activities they provide. This requirement applies to programs, services, and activities provided directly by state and local governments as well as those provided through third parties, such as the American Red Cross, private nonprofit organizations, and religious entities.
Under Title II of the ADA, emergency programs, services, activities, and facilities must be accessible to people with disabilities and generally may not use eligibility criteria that screen out or tend to screen out people with disabilities. The ADA also requires making reasonable modifications to policies, practices, and procedures when necessary to avoid discrimination against a person with a disability and taking the steps necessary to ensure effective communication with people with disabilities.
The ADA generally does not require state or local emergency management programs to take actions that would fundamentally alter the nature of a program, service, or activity or impose undue financial and administrative burdens.
Temporary Medical Facilities
When emergencies arise involving a public health crisis, communities often must provide temporary medical facilities to accommodate the high volume of people requiring medical treatment. Such facilities are sometimes operated by government entities themselves. More often, they are operated by a third party. Regardless of who operates a temporary medical facility, the ADA generally requires facility operations to be conducted in a way that offers people with disabilities the same benefits – e.g., safety, comfort, freedom, medical care, communication, the support of family and friends – provided to people without disabilities.
Because temporary medical facilities may be critical to ensuring the health of people with disabilities in public health emergencies, who are often among the most medically vulnerable, accessibility of these facilities should be a foremost consideration.
Evaluating an Existing Site to Repurpose for Medical Care
It is understandable that in an emergency, thorough pre-planning may be difficult or impossible when time is of the essence. In these cases, accessibility must still be provided to the maximum extent possible.
In instances where existing facilities – e.g., schools, churches, office buildings – are repurposed into temporary medical facilities, steps should be taken to find the most accessible locations and to mitigate existing physical access barriers.
Facilities built or extensively altered since the ADA went into effect in 1992 may have few barriers to accessibility and could be good choices for temporary medical facilities. Facilities built before 1992 and not altered to provide accessibility may have barriers that prevent access to people with disabilities.
Where barriers to accessibility are found in existing facilities, they must be removed, or another nearby accessible facility should be identified. In communities with more than one temporary medical facility, until all facilities are accessible, the locations of accessible facilities should be widely publicized, particularly to people with disabilities and organizations that dispatch patients to temporary medical facilities for treatment.
Important Elements and Common Barriers
The most important accessibility element that should be considered when choosing an existing location to repurpose into a temporary medical facility is the accessible route, which includes entrances.
Accessible Routes are what permit people with mobility disabilities to participate in the services and programs offered during times of emergency. Everyone must be able to get to each of the various areas where services take place. An accessible route should be provided to all critical areas of the medical facility and should be a continuous route between all areas a person might be expected to go. This includes the check-in area, waiting area, examination areas, bed/private rooms, toilet and bathing rooms and discharge area.
Accessible Entrances are part of the accessible route and ensure people with disabilities have a way to get into the facility on a surface that is firm, stable, slip resistant, without steps or steep slopes, and wide enough for a person using a wheelchair or other mobility aid.
Basic Characteristics of the Accessible Route:
- Pathways should be 36 inches wide except at doors and for short distances, when it can be narrower (32 inches).
- Walking surfaces should have a 5% maximum running slope, 5-8.3% maximum for ramps and cross slopes should never exceed 2%.
- Ramps which rise more than 6 inches will need to have both handrails and edge protection, a method which prevents a crutch or wheelchair caster wheel from running off the side of a ramp. Ramps must also have level landings at the top and bottom of each segment and where the ramp changes direction.
- Walking surfaces should be free from gaps greater than ½ inch and vertical changes in level greater than ¼ inch. Vertical changes in level up to ½ inch should be beveled at 1:2. Gaps and changes in level can be caused by broken concrete, potholes along an accessible route, or a threshold at a door.
Common Accessibility Barriers:
Common barriers to accessible entrances and routes can be as simple curbs with no ramps, broken concrete walking surfaces, steps of any number, or even grass on an expected circulation path.
Mitigation strategies should be implemented if such barriers exist. For example, if steps are the barrier to access, a temporary ramp should be installed. A single 6-inch-tall step or curb will require a 6-foot long ramp to act as the accessible route, eliminating that barrier. If an entrance is inaccessible but an alternate entrance is accessible, steps should be taken to direct or assist people with disabilities to the accessible entrance.
Building a New Temporary Medical Facility
Temporary structures can be quickly constructed to accommodate the needs of the community and should be constructed in accordance with ADA Standards. A 36 inch wide circulation path will satisfy accessible route requirements. At least 10% of beds should have a wheelchair space on either side of the bed, and a compliant turning space should be provided within the room. If constructed in a grassy field or otherwise inaccessibly surfaced area, interconnected matting, such as the Mobi-Mat, should be utilized to create an accessible route. If the structure is elevated, a compliant ramp or lift should also be part of the design. Restrooms and showers included in the design should be compliant with the ADA Standards as well. If portable toilets are provided, these should also connect to the accessible route and at least 5% should accommodate people with disabilities.
Additional Considerations
Accessible medical facilities may also contain elements such as public parking, toilets, bathing facilities, and other service areas that need to be examined for barriers.
Some additional general considerations are as follows:
- Medical facilities should have an accessible passenger loading zone (see Figure 1) and accessible parking spaces located in the parking lot nearest the accessible entrance.
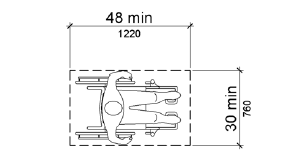
- A 30 inch x 48 inch clear floor space (see Figure 2) should be provided wherever possible at procedural checkpoints associated with a medical exam and hospital stay. If not all examination areas can accommodate this clear floor space, an inventory should be kept on exam spaces which do account for this feature to direct those who require accessibility.
- If a space has inaccessible features, such as multiple floors but no elevator, the inaccessible (upper level) spaces should be filled first by those who are physically able to access them, and the accessible ground floor spaces should be utilized last and be available for patients who require ground level access.
- Reasonable modifications of policies, practices, and procedures must be made to avoid discrimination due to disability, even in times of an emergency. For example, modify “no pets” policies to welcome people who use service animals, unless doing so poses a direct threat to the health and safety of others, which may be the case with a ward of patients with respiratory issues being near animal dander.
Figure 1 - Accessible Passenger Loading Zone
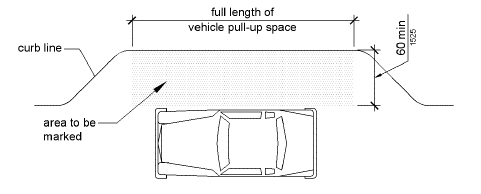
Figure 2 - Wheelchair Clear Floor Space
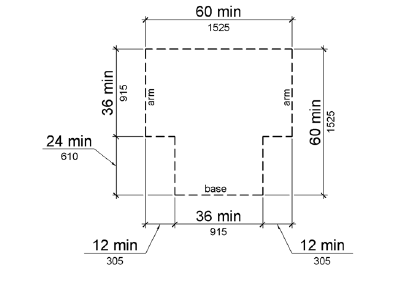
The wheelchair turning space should be either a clear floor circle 60 inches in diameter or a T-shaped space within a 60-inch square with arms and base 36 inches wide. Each arm of the T should be clear of obstructions 12 inches in each direction and the base clear of obstructions for at least 24 inches.